October 2006 archives
October 28, 2006
The Cyclical Ketogenic Diet (CKD) - an overview
20 May, 1995
Breakfast: 4 hard boiled eggs, 100 grams fried bacon, fiber supplement and vitamins
Snack: 100 grams cottage cheese, 10 grams mayo
Lunch: 250 grams minced beef, 80 grams cheese spread with ham, fiber supplement
Snack: 175 grams hard cheese, fiber supplement
Dinner: 240 grams minced beef, 60 grams cheese spread with ham
Supper: 100 grams avocado, 100 grams cottage cheese, 15 grams mayo3,045.5 calories, 10.7 g carbs (1.4%), 244.2 g protein (32.1%), 225.1 g fat (66.5%)
Notes: Starting to feel tired between lunch and the following snack; not too bad (yet). I’m not feeling all that hungry, yet it feels like I haven’t eaten in a long while. Let’s see how it feels like tomorrow after lifting; glycogen stores should be fairly empty by then… [ Excerpt from my nutrition log, the first day on the Anabolic Diet by Dr. Mauro DiPasquale ]
Introduction
 A ketogenic diet is any diet extremely low on carbohydrates, usually below 30 grams a day, which forces the body to take the same steps as in starvation, most importantly that of replacing carbohydrates with fat as the main fuel of the human body. These diets are extreme when compared to the nutrition recommendations in vogue, but the fears surrounding what a diet rich in fats and protein could do to us have proven largely ungrounded (as a sideline, diets rich in fats AND carbohydrates are a whole different story and should not be confused with low-carbohydrate high-fat diets as the biochemistry behind them is radically different). Much of the data on the safety of this diet comes from the clinical use of ketogenic diets to control childhood epilepsy where children are kept for years on this kind of diet with little side-effects. Nevertheless, it should be recognized that the amount of long-term research data is still scant. The debate surrounding whether our stone age ancestors lived mostly on a ketogenic diet or not (which would point to us still being biologically primed for that kind of fare) is still out in the open, but the fact remains that there are good examples of people, most notably the Eskimoes and Northern Europeans during the harsh winter months, that subsided mostly on a fare of meat and fat while having very low incidence of cardiovascular diseases. Be that as it may, this overview of a particular ketogenic diet is not geared towards defending the diet nor towards proving how this is the only way to lose fat efficiently (it’s not), but rather to present how the diet works biochemically and how it is done in practice. Towards that end, there is no attempt to fully reference the claims made in this article; those who want to examine the research behind ketogenic diets should start by reading the fully referenced The Ketogenic Diet - A Complete Guide for the Dieter and Practitioner by Lyle McDonald, without doubt THE defining work on the topic of using the diet for athletes; every serious ketogenic dieter should own a copy. For information on how the diet is used in treating childhood epilepsy, see The Epilepsy Diet Treatment: An Introduction to the Ketogenic Diet by Dr. Freeman et al. and the factual movie First Do No Harm.
A ketogenic diet is any diet extremely low on carbohydrates, usually below 30 grams a day, which forces the body to take the same steps as in starvation, most importantly that of replacing carbohydrates with fat as the main fuel of the human body. These diets are extreme when compared to the nutrition recommendations in vogue, but the fears surrounding what a diet rich in fats and protein could do to us have proven largely ungrounded (as a sideline, diets rich in fats AND carbohydrates are a whole different story and should not be confused with low-carbohydrate high-fat diets as the biochemistry behind them is radically different). Much of the data on the safety of this diet comes from the clinical use of ketogenic diets to control childhood epilepsy where children are kept for years on this kind of diet with little side-effects. Nevertheless, it should be recognized that the amount of long-term research data is still scant. The debate surrounding whether our stone age ancestors lived mostly on a ketogenic diet or not (which would point to us still being biologically primed for that kind of fare) is still out in the open, but the fact remains that there are good examples of people, most notably the Eskimoes and Northern Europeans during the harsh winter months, that subsided mostly on a fare of meat and fat while having very low incidence of cardiovascular diseases. Be that as it may, this overview of a particular ketogenic diet is not geared towards defending the diet nor towards proving how this is the only way to lose fat efficiently (it’s not), but rather to present how the diet works biochemically and how it is done in practice. Towards that end, there is no attempt to fully reference the claims made in this article; those who want to examine the research behind ketogenic diets should start by reading the fully referenced The Ketogenic Diet - A Complete Guide for the Dieter and Practitioner by Lyle McDonald, without doubt THE defining work on the topic of using the diet for athletes; every serious ketogenic dieter should own a copy. For information on how the diet is used in treating childhood epilepsy, see The Epilepsy Diet Treatment: An Introduction to the Ketogenic Diet by Dr. Freeman et al. and the factual movie First Do No Harm.
The first part of this article attempts to explain the biochemistry behind how ketogenic diets work without previous knowledge of fuel metabolism. Doing so, the case is presented in an order somewhat different from that found in many textbooks (as a case in point, insulin is left to the end of the discussion). The text is kept as brief as possible, but central concepts have external links, mostly to Wikipedia for laziness’ sake, for those readers who would like to face the biochemical nitty-gritties. There is also a cursory link section at the end of this article. Still, nothing beats getting a good introductory biochemistry book if you want to see the big picture. Starvation and fuel metabolism have been well-studied and the biochemistry behind a ketogenic diet is largely uncontroversial. The second part of the article distances itself from the theory and shows how to set up a modified ketogenic diet with carb loading to meet the needs of athletes involved in strenous anaerobic activities such as heavy weight training.
This article draws heavily on a 1997 article I wrote in Swedish on the cyclical ketogenic diet based on the lively discussions on the lowcarb-l mail list (you can find my posts via the archives search engine if you enter Lindqvist Kristoffer J as author), Mauro DiPasquale’s Anabolic Diet manual and video from 1995, and the bits and pieces of information available on the web at the time (the most important being the BodyOpus archives by Lyle McDonald). Ultimately, much of the credit for pulling together the research and polishing up the diet belongs to Lyle McDonald and Jeffrey Krabbe, who were the leading men when this variation of the diet was being formulated on the lowcarb-l list. In the end, Krabbe pulled out of their joint book project leaving McDonald as the sole author of the aformentioned The Ketogenic Diet which refined the theory of the earlier works on cyclical ketogenic diets, notably The Anabolic Diet by Dr. Mauro DiPasquale (actually, as we will see later, this diet is not strictly speaking ketogenic) and BodyOpus by Dan Duchaine. This article has been checked and revised against the first edition of The Ketogenic Diet (1998) together with a close reading of some of the biochemistry books in my bookshelf. To my knowledge not much has changed since the late 1990s, but I naturally welcome any updates or corrections you may have (comments can be left at the end of the article). My own experience with this diet goes back to 1995 (two months), 1996-1997 (lived on it for well over a year with only a few carb weeks here and there) and 2002 (six-weeks) in conjunction with bodybuilding style training. As this article goes to press, I am on my sixth week of the diet for the purpose of dropping fat weight off for a virtual powerlifting meet. Before we roll, let me emphasize that I take no responsibility for anyone following any advice found in this article. Curtains up!
Part I: The theory behind ketogenic diets
A CRASH course on the biochemistry behind starvation and ketogenic diets
The human body needs energy to function. Ultimately, the source of all energy (calories) is the food you eat - specifically the digestable carbohydrates (carbs for short), proteins and fats your meals contain. The digestive tract extracts these nutrients from the food that passes through it and splits them into smaller fragments usable to the cells before they can enter the bloodstream; carbohydrates are split into simple sugars (mainly glucose), protein into amino acids, and fats into glycerol and fatty acids. Out of these, humans can extract 4 calories from each gram of protein, 4 calories from each gram of carbs and 9 calories from each gram of fat [note that this article uses calories in the colloquial sense; technically, we should say kilogram calories (kcal)].
The problem is, these fuels enter the body discontinously as you eat every few hours, yet the body continously needs energy to function. It is not physically possible for the body to keep all the nutrients it has floating around in the bloodstream, hence it needs to warehouse the excess somewhere where it is accessable between meals and during sudden rises in energy demand (such as during strenous exercise). Glucose is stored as glycogen in the muscles and liver. Fatty acids end up mainly as triglycerides (also called triacylglycerols) together with glycerol (specifically, one molecule of glycerol binds to three molecules of fatty acids) in the fat cells of adipose tissue located under the skin and around the internal organs, where it acts as insulation and padding, although some triglycerides are also present in all cells. In contrast, amino acids cannot be stored beyond a small pool in the bloodstream, and are used immediately for a variety of tasks - including structural repair of muscle tissue and acting as catalysts, carriers and receptors in various processes. When there are more amino acids available than can be used, the excess is converted into glucose or fatty acids as needed. Similarly, once the glycogen stores are full, any excess glucose is converted into fatty acids for storage. In a nutshell, the triglyceride deposits will readily absorb any excess of amino acids or glucose and can theoretically grow as large as the body can carry without collapsing. In the human body, fat is the ultimate form of stored energy. Fats carry more than double the calories per gram than glucose (i.e., 9 calories per gram for fats vs. 4 calories for glucose) and does not need to bind to water to be stored, unlike glucose where every gram of glucose binds to approximately 2.7 grams of water to form glycogen. This means that stored fats yield 9 calories per gram whereas glycogen only yields 1.33 calories per gram. To give you some perspective, if you stored the energy found in 10 lbs/5 kg of fat as glycogen it would amount to 67.5 lb/31 kg. In practice, the energy of all stored glycogen never exceeds 2,000 calories (the average under normal conditions being less than 1,000 calories) whereas someone carrying 33 lbs/15 kg of stored fat (eg. a 150 lb/68 kg man with 22% bodyfat) would have 135,000 calories worth of energy from fat alone!
Most human tissue prefers glucose as fuel over fatty acids, but some tissue (including the brain and Type II muscle fibers) are unable to use fatty acids for energy at all. When glucose is available it is always the preferential fuel, with fat deposits functioning as a large store of backup energy for those times when food might not be available in sufficient quantities. Yet, glycogen stores are too small to last for more than a day unless refilled. Furthermore, glucose can only enter muscle, not exit back into the bloodstream. Muscle glycogen can only be used to fuel the muscle it is stored in, thus leaving liver glycogen as the sole source of readily available stored glucose for all other tissue. There is some variability based on meal size and composition, but as a general rule of thumb the liver needs to start converting its glycogen back to glucose and eject it into the bloodstream (called glycogenolysis) within four hours of a carb containing meal. Unless more carbs are ingested, only the tissue totally dependent on glucose will be able to absorb available glucose with other tissue having to turn to breaking down fatty acids for energy. As glucose levels in the blood continues to fall, the body initially tries to counter this by converting other available fuels to glucose. In animals, fatty acids cannot be converted into glucose, but glycerol can be. However, glycerol alone is not enough which causes an increasing amount of amino acids (mainly alanine and glutamine) to be converted into glucose (gluconeogenesis) in the liver, and to a lesser extent in the kidney, which practically means that muscle tissue is broken down for energy.
Within 16 hours after the last carb containing meal, liver glycogen is almost depleted and blood glucose levels adequate to fuel the brain and other glucose dependent tissue can no longer be maintained solely by breaking down amino acids. At this point, the brain would slowly cease functioning and go into coma if there would be no alternate way of producing the fuel it needs. Luckily, the liver has one more trick up its sleeve called ketogenesis. Even in the presence of carbohydrates, the liver is always producing something called ketones out of free fatty acids, although in too minute amounts for them to be of much physiological consequence. However, once liver glycogen is depleted, ketogenesis is rapidly increased. As it turns out, most tissue in the body will happily use ketones for energy when glucose is not available, including those unable to use fatty acids; thus, glucose and ketones are both nearly universally accepted fuels for the whole body whereas several kinds of tissue can’t work with fatty acids. As the brain gradually adapts to using ketones as fuel over about three weeks of ketosis (the state where the body uses ketones as its main fuel instead of glucose) it will happily replace up to 75% of its glucose requirements with ketones. As glucose requirements are drastically reduced, the amount of amino acids that need to be converted into glucose also decreases sharply. Thus, like glucose, ketones have a protein sparing effect. If protein would continue to be broken down at the rate seen before the body has fully adapted to ketosis, a starving individual would quickly run out of muscle mass and die (being unable to move due to muscle athropy long before that); thanks to the lowered conversion rates, it is the size of the fat deposits that matters thus allowing an average individual to survive for months. Even when in ketosis, the brain still requires roughly 40 grams of glucose per day, but this amount is easily met by conversion of amino acids and glycerol to glucose. As a sideline, the initial breaking down of muscle tissue also serves as an important adaptation to starvation as less muscle mass means that less calories are needed to sustain the body.
In sum, the state of ketosis appears to essentially be a survival mechanism that ensures that the brain gets what it needs when glucose is sparse (to think of a way to obtain food) by producing an alternative fuel source, ketones, out of our largest energy deposits (fat) to appease the other types of tissue normally dependent on glucose. Ketosis also has the effect of blunting hunger which could easily stand in the way of hunting for food. Thanks to ketosis, extremely obese persons can survive for over a year with no food as long as water and the various mineral/vitamin requirements are met (this has been done clinically to diet down people who face urgent health issue due to their extreme weight at the cost of a large loss of lean body mass - do NOT try this at home).
A ketogenic diet mimics starvation by lowering carbohydrates, thus causing ketosis. The main difference is that as adequate protein is eaten, the body will use that to produce glucose instead of having to break down muscle tissue. Furthermore, whereas starvation sucks the minerals it needs from wherever it can find it in the body (such as in the bone structure), a ketogenic diet again supplies them through diet and supplementation. On paper this sounds like the ultimate diet for fat loss. Fat is the main source of fuel and, unlike what often happens on a carbohydrate based diet when carbs are too low or not ingested frequently enough, protein theoretically never needs to be broken into glucose as long as the body doesn’t run out of fat (very unlikely) and protein is eaten in enough quantities. As fats take longer to digest and ketosis blunts hunger, the sensation of hunger is much lower than on a carbohydrate based diet despite the volume of food being much lower on a ketogenic diet. In ketosis the body is a fat burning machine, when not in ketosis (as on a traditional carbohydrate based diet) the body is primarily a glucose burning machine supplemented by some fat if calories are below maintenance.
The case for carbohydrates
Properly executed, ketogenic diets would appear to indeed save lean body mass better than traditional carbohydrate diets. As we have seen, the body does not actually need carbs to function BUT the absence of carbs does come at a price for a weight training individual.
To understand the role of carbohydrates we need to say a few words on HOW the body regulates blood glucose levels. This happens with the help of two hormones. When blood sugar levels rise, such as after a meal, it causes the pancreas to secrete a hormone called insulin which stimulates the storage of glucose as glycogen (and fat once the glycogen stores are filled). Insulin also stimulates protein synthesis and pushes amino acids into the muscle cells (or, again, fat stores if no aminos are needed for repair or other functions). Conversely, as blood glucose levels drop so does insulin levels. This, in turn, causes another hormone, glucagon, to be secreted by the pancreas. Glucagon does the opposite thing as insulin, namely stimulates the release of stored fuels (liver glycogen, triglyceride stores and protein breakdown) to the degree necessary to restore normal blood sugar levels. Thus, insulin is an anabolic (”building up”) hormone whereas glucagon is a catabolic hormone (”breaking down”). Very plainly put, what determines whether insulin or glucagon predominates is simply the amount of glucose in the blood (blood sugar levels). Now, carbs, protein and fats are all converted to glucose to some degree and so all affect blood sugar levels, but to different degrees. Basically, carbohydrates will be 100% converted to glucose, protein 54% and fat 10% (from the glycerol part) regardless of whether the body is in ketosis or not. This means that carbohydrates have the strongest influence on blood sugar levels by causing a much larger insulin response than protein or fats. Put simplistically, a carbohydrate based diet will cause insulin to predominate thus priming the body for repair and fuel storage whereas a diet low in carbohydrates will cause glucagon to dominate thus promoting the breakdown of stored fuels while inhibiting muscle repair. It should be fairly obvious where this is going: the benefit of a low carbohydrate diet, specifically a ketogenic diet, is the stimulation of fat breakdown via high glucagon levels, but the low levels of insulin makes muscle repair suboptimal compared to a carbohydrate based diet. What happens on a carbohydrate diet is the opposite, namely that muscle repair is stimulated but fat loss inhibited (this is one of the reasons why it is so hard to naturally gain muscle mass without also gaining fat as insulin promotes both processes in the body). Blood sugar levels are essentially identical on carbohydrate diets and ketogenic diets, but the hormonal environment that ensures this is much different.
Secondly, type II muscle fibers require glucose to function optimally. Type II muscle fibers are the so-called white or fast twitch muscle fibers that are primarily used during anaerobic activities, such as heavy weight training and sprinting. Recall that the depletion of liver glycogen is what ultimately causes ketosis. Even when in ketosis, the type II fibers will receive the glucose it needs to work optimally for as long as the muscle glycogen stores are not depleted. Once the stores are empty, such as after a single workout of sufficient volume, the muscle has to rely on fatty acids and amino acids broken down into glucose thus causing performance to drop.
As you can see, a long-term ketogenic diet (such as Atkins) comes at a heavy price for anyone training with weights or involved in anaerobic activities. This is why strength athletes ultimately need carbs to reach peak performance and why ketogenic diets geared towards athletes generally include well-timed carbs in some capacity; carbs are usually eaten either around workouts (Targeted Ketogenic Diets, TKDs) or during 24 to 48 hours once a week or less (Cyclical Ketogenic Diets, CKDs). The carbohydrates will disrupt ketosis, but will cause a brief anabolic insulin spike that replenishes muscle glycogen and promotes muscle repair. When well-timed, the trainee quickly returns to ketosis (in fact, on TKDs ketosis is not necessarily even disrupted). The rest of this article will focus on CKDs, which arguably are superior to TKDs for serious lifters.
On a CKD, glycogen stores are first depleted by weight training and then refilled all at once using a high carbohydrate intake that will take the dieter temporarily out of ketosis before the low-carbohydrate fare is resumed - this is very similar to the classical carbohydrate loading model employed by marathon runners which causes muscle glycogen stores to become supercompensated (as in much bigger than normal, on the order of 150% following a 36 hour carb-load, provided enough carbs are ingested). Glycogen supercompensation will only occur if the muscle glycogen is depleted enough, hence it is imperative that enough muscular work (weight training) is performed before the carb-load (more details to follow). The reason a 24-48 hour carb load is used is that only so much glycogen can be resynthetised per hour. The amount of carbohydrates that must be ingested is large, around 4.5 grams of carbs per pound/10 grams of carbs per kilogram LBM for the first 24 hours, but with muscle glycogen being depleted, the risk of fat gain is minimal until the deposits are filled to the brink. This is a big boon psychologically, as at least twice the amount of calories are ingested for the first 24 hours compared to the low-carb days and all the carbohydrate-dense foods that are totally off-limit during the low-calorie low-carb days can now be eaten (even candy is desirable at the beginning of the carb load). Physiologically, the brief spike in calories also shakes up the metabolism thus preventing the body from going into the fuel sparing mode which often happens when calories are kept below maintenance levels for long periods of time.
In practice, these modifications have proven successful means of retaining performance in the gym while effectively sparing muscle tissue and reaping the benefits of ketosis, BUT the fact remains: the constant presence of insulin on a carbohydrate containing diet is superior for building lean body mass everything else being equal. In a nutshell: a well-orchestrated ketogenic diet is likely to be superior for shedding fat while retaining as much muscle mass as naturally possible, but it is not the way to huge gains in muscle or strength. This is why it is common to cycle ketogenic diets for fat loss with carbohydrate based diets to build muscle with some gains in fat. Some athletes might find the ketogenic a valuable aid in those circumstances where some strength or muscle gains are desired while keeping bodyfat gains to a minimum.
How much fat, protein and carbs should one eat on the low-carb days?
As should be clear by now, the maximum carbohydrate intake allowable on the low-carb days is simply one that does not prevent ketosis. On a CKD, where the number of low-carb days are limited due to the carb load, it is important that carbs are kept low enough to ensure that the dieter enters ketosis reasonably fast (ideally within 36-48 hours). The amount of carbohydrates that can be tolerated depends on the individual, whether ketosis has been established or not (more carbs can generally be tolerated once in ketosis), and whether the body has fully adapted to using ketones as fuel. A maximum of 30 grams per day is a good rule of thumb, but experimentation is key. We have also seen that the body can produce all the glucose the brain needs from breaking down amino acids, so no carbs are required on the diet per se, but they help make food choices less monotonous and allow the inclusion of natural fiber rich vegetables (more on this below).
The minimum protein intake is in turn determined by what is needed to keep the muscle from having to turn to breaking down muscle protein. Studies referenced in The Ketogenic Diet (pp. 56-60) suggests that as little as 120-150 grams of protein per day regardless of calorie levels is enough to prevent muscle protein breakdown in sedentary individuals. Regardless of diet, weight training individuals require more protein to meet the increased need to repair the structural damage caused by training. Furthermore, on a ketogenic diet additional protein is needed during the first three weeks or so as more protein is converted to glucose before the body fully adapts to using ketones as fuel. A general recommendation is to consume between 0.9-1 gram per pound/1.9-2.2 grams of protein per kilogram of LBM (lean body mass, i.e. bodyweight minus fat weight) for the first three weeks OR 150 grams, whichever is higher. After full adaptation has taken place, protein intake could be lowered somewhat to a minimum of about 0.8 grams per pound/1.75 grams per kilogram of LBM. Using total bodyweight instead of LBM is all right for leaner individuals, but more obese subjects should, if possible, base protein intake on an accurate measurement of LBM as the additional bodyfat might lead to a sizable excess of protein. As even caliper measurements are not 100% reliable, individuals basing protein requirements on LBM calculated by that means should probably overestimate slightly to ensure adequate protein intake (when in doubt, always err towards too much protein rather than too little). Also, since we know that 54% of all ingested protein will appear as glucose in the bloodstream compared to 100% for carbs, we can note that for every gram of carbs ingested protein intake goes down by two grams.
A more trickier question is whether there is a maximum allowable intake of protein and what role fats play on a ketogenic diet. If the body can extract all the energy it needs from stored body fat there would seem to be little use for fat in the diet. If anything, fat intake would seem to counterproductive as the body would first use the dietary fat for energy before tapping into stored fat. The more fats are ingested, the less body fat is burned. Why not keep fats and carbs down and use an all-protein diet?
Actually, there are diets out there that do just this, the most sensible of which appears to be none other than Lyle McDonald’s The Rapid Fat Loss Handbook (Amazon link), a variation of the Protein Sparing Modified Fast (PSMF). This diet cuts everything out except protein and some very low calorie vegetables, essentially reducing caloric intake to the amount of protein needed to prevent muscle mass loss; for most people this will mean a miniscule 600 to 1,000 calories a day! What is burned is almost exclusively body fat and that at quite an impressive rate too. So why not go with that? First of all, the low amount of calories will signal to the body that there is a serious food emergency to which it will respond by shifting into an energy saving mode where energy is spared by slowing down all possible processes of the body; the result of this metabolic slowdown is lowered energy needs causing fat breakdown to slow down significantly (this is why dropping calories too low will result in less fat loss). The diet does include periodic breaks (single meals or longer refeeds) to offset this, but this is still an issue. Added dietary fat simply helps keep the calorie count up which will do much in keeping the metabolism active provided calories are not dropped too low. The very low calorie count will also make it very difficult to sustain any kind of heavy training and will more than likely make your life seem like a living hell, even if that hell is one heck of a fat burning machine. McDonald makes it very clear that this is a CRASH diet that should only be followed for very short periods of time in emergencies where weight needs to be shed very quickly (a lot of water weight will accompany the fat loss). No crash diet is ultimately a healthy diet and difficulties keeping the weight off long-term after such a regime is also an issue. If you want to try this, definitively read McDonald’s book first. Done wrong, this kind of diet can potentially kill you.
Secondly, fat helps promote ketogenesis. We saw above that 54% of all ingested protein will be turned into glucose (compared to 100% for carbs and 10% for fats). If protein levels are excessive, it can lead to an excessive production of glucose (and thus raised insulin levels) that will prevent ketosis. Conversely, much less glucose is produced when more calories come from fats. We can thus say that carbs are anti-ketogenic (prevents ketosis) and fats ketogenic (promotes ketosis) with protein being mildly anti-ketogenic. When ketogenic diets are used in the treatment of epilepsy, the ratio of grams fat to grams protein plus grams carbohydrates (ketogenic ratio) is kept between 2:1 and 5:1 which will stimulate deep ketosis (for yet unknown reasons, ketone concentration needs to be high to prevent seizures which is also why water intake is restricted for epileptics). Epilepsy research tells us that 1.5:1 is about as low as most people can go in order to produce ketones (lower ratios are known to work for some, especially those who have been on a ketogenic diet for an extensive period of time). Worked out as fat percentage of calories, 1.5:1 adds up to 77% fat (2:1 is 81% fat and 5:1 91% fat). Importantly, this research is based on individuals not engaged in exercise which helps keep blood glucose levels down. A case in point is that individuals engaged in heavy weight training often have no problems establishing ketosis following 1:1 levels, i.e. 69% fat, or even less. The lower the ketogenic ratio is dropped, the more exercise will matter and the more individual differences will become visible. Bodyopus recommends a 75% fat ratio which adds up to 1.3:1, also below the 1.5:1 rule of thumb.
Recently, the importance of establishing ketosis has also been questioned. Lyle McDonald has stressed that adequate protein intake should never be sacrificed for ketosis. A similar sentiment is echoed by Chris Shugart and TC Luoma in their article on the T-Dawg Diet version 2.0, where they see the benefits of ingesting a carbohydrate containing postworkout drink outweighing the importance of uninterrupted ketosis. As a matter of fact, the Anabolic Diet is not even designed to be a ketogenic diet, and should rather be labeled a low-carbohydrate or high-fat diet. The 55-60% fat intake the Anabolic Diet recommends works out to a ketogenic ration of 0.6:1 to 0.7:1 (note that this is either misquoted by Lyle McDonald in his BodyOpus notes where he states that the Anabolic Diet recommends 65-70% fat calories OR was changed after the 1995 edition I own); this ratio is already mildly anti-ketogenic and, together with the 30 grams of carbs, is designed to keep the trainee OUT of ketosis. In practice, this might not be enough for everyone though. In a 1999 interview, DiPasquale states very clearly his opinion that ketosis is actually very catabolic and that just dropping carbs very low while keep the aforementioned fat ratio will cause the “metabolic shift” where the body becomes a fat burning machine while avoiding the evils of ketosis.
At this point, the research does seem to point to some advantages of ketosis, but it might not be as important for dieting as originally thought. A tentative suggestion is to worry first about protein and only then about ketosis. In sum, manipulating the ketogenic ratio upwards (more fat, less protein + carbs) is a good place to start when troubleshooting problems with establishing ketosis as long as protein is kept adequate to migitate muscle loss, i.e. not going below 0.8 grams pound/1.75 grams kilogram LBM. For epileptics the priority is the opposite; high ketone concentration is what prevents seizures and, as a consequence, some lean body mass loss due to the low level of protein intake of a high ketogenic ratio is acceptable. In fact, some people do report better results on the Anabolic Diet (my experience is the opposite though) and it might be worth trying both diets to compare results. Whether ketosis is desirable or not may be debated, but at least it seems clear that deep ketosis is not something a dieter should aim for as lower ketone concentrations seems to lead to better fat loss anecdotally. What is also clear is that a ketogenic diet works well; in the end the whole discussion about ketosis vs. no ketosis on a low-carbohydrate diet may turn out to be a moot one. Ketosis is also a reliable indicator that the diet has indeed started to use fat as the primary fuel and is as such a valuable feedback mechanism.
Should I use a ketogenic diet to diet down then?
Not necessarily. Anecdotally, for some a ketogenic diet is a disaster and they do much better on a traditional carbohydrate diet. It is also my belief that what is optimum has to do with much more than whether the diet itself is effective, including social and personal motivations as well as willingness to accept the side-effects of this diet. Side-effects include smelly breath when in ketosis (ketones are excreted in the breath as well), having to avoid the ever-present carbohydrates so tied to social life in our society and having to structure training around the diet (more on this below). The diet can also be hell until the brain adapts fully to using ketones as fuel causing diziness, mental lethargy and a feeling of near constant hunger (the worst usually passes in a few days, but symptoms may last for two to three weeks especially on the CKD due to the carb load slowing down the adaptation some) - Dr. DiPasquale goes as far as recommending against running heavy equipment during the first week. The only way to find out if this diet works well for you is to endure the transition to a ketone metabolism, i.e. the first three weeks. Ketogenic diets are also not the way to go without extensive medical consultation for pregnant or breastfeeding women, children or persons with certain illnesses including diabetes and kidney disorders. People prone to eating disorders should probably also stay away from the cyclical ketogenic diet, as the carb-load that follows several days of low-calorie low-carb eating is very similar to a food binge. The diet does appear to be as safe as any diet, but if you constantly feel alarmed of what it might do to your cholesterol, blood pressure or whatever, you will probably want to look at other alternatives. Potentially, the diet also carries many benefits including better fat loss, less allergies (reported by many) and a more stable mood as you get off the insulin rollercoaster (not to mention the almost total lack of constipation on the low-carb days… the carb load is another story…). Personally, I have much more energy on a ketogenic diet and feel mentally clearer which is one of the main reasons I lived on one for well over a year.
Part II: The cyclical ketogenic diet (CKD) in practice
Preliminaries
Get a good scale especially if the one in your bathroom has a tendency to show different values depending on how you stand on it. Many home scales are not very accurate (as can be seen when comparing several of them against each other), but what is most important is that they are consistent so you can track your relative weight loss (i.e. going from 103kg to 100kg and going from 101.5kg to 98.5kg both equals 3kg no matter if your scale is correct or not).
Have your bodyfat measured using either calipers (cheap) or underwater weighing (expensive). Stay away from all kinds of electronic bodyfat devices as they are notorious for being off the target especially for subjects who carry above average levels of muscle mass. It takes a lot of practice to become proficient at caliper measuring, so select your expert carefully and make sure to ask the same person to take follow-up measurments to ensure consistent measuring. The scale is simply not enough on its own as it doesn’t differentiate between whether the lost weight was muscle or fat. Tracking bodyfat levels, you can accurately state the ratio of lost muscle to fat. This is ultimately the best way to know whether the diet did it’s job well or not. If you lost 20 lbs/9 kg, the majority of which was hard-earned muscle, your diet was clearly a disaster no matter how impressive it looks by scale.
At a minimum, arrange to have your cholesterol (total cholesterol as well as HDL and LDL) measured before embarking on the diet. The ratio of “good cholesterol” (HDL) to “bad cholesterol” (LDL) generally improves on the CKD, but there are exceptions and you really need to know how the diet impacts your cholesterol as this can have a tremendous impact on your overall health. Just make sure not to take a second test before a few months have passed, cholesterol levels are known to sometimes increase in the beginning of a radical diet change according to a doctor I spoke to. Preferably, do a complete health check-up. Better knowledgeable than sorry.
 Buy Ketostix from your local pharmacy to measure ketone levels in your urine. Just pee on them, wait for 15 seconds and compare the color against the chart on the bottle; the picture shows a negative result (beige color) and a positive trace ketones result (light pink). The darker the strip, the higher the ketone concentration. Ketostix are not necessary for experienced ketogenic dieters, who can easily tell whether they are in ketosis or not from how they feel and the metallic taste in their mouth, but are essential for beginners. Ketostix help monitor how quickly ketosis is established, and is an invaluable tool in determining how many carbohydrates you can tolerate without being thrown out of ketosis and in troubleshooting reasons for not becoming ketogenic (such as artificial sweeteners which affect some people but not others). Just be aware that Ketostixs are not 100% reliable since they only measure EXCESS ketones spilling into the urine (urinary ketosis) and are sensitive to hydration levels (drinking a lot will naturally dilute the ketone concentration in the urine) - it is very possible to be in ketosis even with no traces on the sticks. The only reliable way to assess the level of ketosis is to measure ketone concentrations in the bloodstream; some blood glucose meters used by diabetics can do this. That kind of accuracy is rarely needed on a ketogenic diet, but for a diabetic rising ketone levels are a potential life and death situation. The depth of ketosis people enter also varies a lot from person to person. In theory, fat loss is best with only traces of ketones so don’t make it a hobby to try to reach very deep colors! Ketostix are an important tool, but don’t invest all your emotion into them.
Buy Ketostix from your local pharmacy to measure ketone levels in your urine. Just pee on them, wait for 15 seconds and compare the color against the chart on the bottle; the picture shows a negative result (beige color) and a positive trace ketones result (light pink). The darker the strip, the higher the ketone concentration. Ketostix are not necessary for experienced ketogenic dieters, who can easily tell whether they are in ketosis or not from how they feel and the metallic taste in their mouth, but are essential for beginners. Ketostix help monitor how quickly ketosis is established, and is an invaluable tool in determining how many carbohydrates you can tolerate without being thrown out of ketosis and in troubleshooting reasons for not becoming ketogenic (such as artificial sweeteners which affect some people but not others). Just be aware that Ketostixs are not 100% reliable since they only measure EXCESS ketones spilling into the urine (urinary ketosis) and are sensitive to hydration levels (drinking a lot will naturally dilute the ketone concentration in the urine) - it is very possible to be in ketosis even with no traces on the sticks. The only reliable way to assess the level of ketosis is to measure ketone concentrations in the bloodstream; some blood glucose meters used by diabetics can do this. That kind of accuracy is rarely needed on a ketogenic diet, but for a diabetic rising ketone levels are a potential life and death situation. The depth of ketosis people enter also varies a lot from person to person. In theory, fat loss is best with only traces of ketones so don’t make it a hobby to try to reach very deep colors! Ketostix are an important tool, but don’t invest all your emotion into them.
Make up a plan for how you will measure your calories. Based on research that shows that ketogenic diets usually cause people to eat less than on a carbohydrate based diet (due to the blandness of the fare, the high amount of fat that slows digestion and the general appetite blunting associated with the diet), some proponents (such as the late Dr. Atkins) makes a case for just eating as much as you want, even when targeting fat loss, as that should be less than what you would normally eat anyway. This might be the case generally, but unfortunately this has given rise to the notion that one can eat “unlimited amounts of fat and protein”. Eat too many calories on any diet, and you’ll pack it on (it is a myth that all excess calories on a ketogenic diet are lost in the urine, the ketones that are lost in urine represent very negligible calories). That’s just basic physiology as explained earlier. Foods heavy on fat are very calorie dense; it is easy to overeat stuffing yourself with oils, bacon and whatnot - especially if you are an athlete with a healthy appetite. On the flip side, some people will eat way too little causing metabolism to slow down and the tearing down of muscle protein for glucose. If you are an athlete, you really MUST track your calorie levels which is really the key to fine-tuning the diet through adjusting calorie levels and the ketogenic ratio as needed based on the feedback received from the scale, bodyfat measurements and the ketostix. What you need is a good food scale (no, this doesn’t have to mean an expensive electronic model), food nutrition tables appropriate to the part of the world you live in (many countries have this information online, an example being Fineli maintained by the National Public Health Institute of Finland) and familiarizing yourself with how to count calories and calorie ratios. A good piece of software, such as FitDay, can help a lot as well as speed up things tremendously.
Inform your near friends and family about the diet so you and they don’t end up in awkward situations involving food. If you want to be really hard on them, just give them the link to this article… Remember that not everyone knows what a carbohydrate is and what low-carb food is.
Stock up on the basic vitamins/minerals (at least multi-minerals, magnesium and vitamin C) and foods you will need, such as high-quality oils, meat in the freezer, eggs, cheese, bacon, some kind of fiber containing vegetables (see below), cream and so on and so on. You might get good deals if buying some ingredients, such as eggs, in bulk. You might also consider purchasing one of the Atkins cookbooks or peruse the web for low-carb recepies. These make a world of difference if you find the diet getting very bland. Low-carb bread? Yes, and it’s tasty too. ![]()
Plan your weight training and other related activities (cardio if you must…) around the diet and decide on what days in the week you will do the carb-load. The specifics are discussed below.
Setting up the diet
Food intake on the low-carb days
The rationale behind the ratio of carbs, protein and fat has been discussed above. Basically: carbohydrates need to be limited to about 30 grams/day to stimulate ketosis and protein needs to be high enough to prevent the breakdown of muscle protein that is associated with ketosis through starvation. With carbohydrate and protein intake being relatively fixed from day to day, calories are adjusted by manipulating the amount of fat you eat. There are more esoteric ways of working out the macronutrient (protein-carb-fats) ratio, but this formula generally works well with some tweaking as you go. However, it should be noted that if you drop calories low enough to cause the percentage of calories from fat to drop below about 65% you might have trouble entering ketosis and might need to increase fat while lowering carbs and/or protein.
- Determine calories: start at 12-13 calories per pound/26-28 calories per kilogram of bodyweight and lower moderately as needed to sustain 1-2 lbs of fat loss/week. Calorie levels under 1,200 or 9 calories per pound/20 calories per kilogram should be avoided as the slowed down metabolism will quickly cause fat loss to come to a grinding halt.
- Determine protein intake based on either lean body mass (especially heavier individuals) or total weight. For the first three weeks, use between 0.9-1 gram per pound/1.9-2.2 grams of protein per kilogram OR 150 grams, whichever is higher. After three weeks, protein intake could be lowered somewhat to a minimum of about 0.8 grams per pound/1.7 grams per kilogram.
- Determine carbohydrate intake: a good rule of thumb is to keep the daily intake to below 30 grams. That said, the amount of carbohydrates needed to affect ketosis show large fluctuation between individuals and depends on how deep ketosis you are in. You might want to keep carbs very low until you are safely in ketosis and then raise your intake somewhat. Experimentation coupled with ketostix is key here. For now, stick with below 30 grams/day.
- Determine fat intake by subtracting the sum of calories from protein and carbs from your total caloric intake (recall that every gram of protein and carbs yield 4 calories, whereas fat yields 9 calories per gram). Fat simply makes up for the calories that are left after protein and carbs have been determined.
Here’s an example for a 209 lbs/95 kg individual just starting on the diet for fat loss. For clarity, the example is in pounds only.
- Calories: 209 lbs bodyweight * 13 calories per pound = 2,717 calories
- Protein: 209 lbs bodyweight * 1 gram protein per pound = 209 grams. This is 209 grams * 4 calories per gram of protein = 836 calories.
- Carbs: 30 grams. This is 30 grams * 4 calories per gram of carbs = 120 calories.
- Fat: Protein and carbs make up 836 protein calories + 120 carb calories = 956 calories. Fat should make up the rest, i.e. 2,717 total calories - 956 calories = 1,761 calories. Since every gram of fat contains 9 calories, this means 1,761 calories / 9 calories = 195 grams of fat.
This results in a diet consisting of 4.4% carbs (120 * 100 / 2717), 30.8% protein (836 * 100 / 2,717), and 64.8% fat (1,761 * 100 / 2,717). The ketogenic ratio is 195 grams of fat to 209 grams of protein + 30 grams of carbs, i.e. 195 / 209+30 = 0.8:1. If this individual has trouble establishing ketosis, carbs and protein could be cut slightly to produce a better ketogenic ratio as long as protein does not go below 0.8 grams per pound, i.e. 0.8 * 209 lbs = 167.2 grams. As noted, protein should not be cut drastically during the first three weeks until protein requirements go down due to adaptation to ketosis.
Food intake during the carb-load
As we have seen, the purpose of the carb load is to refill muscle glycogen, shake the metabolism by raising calories and to cause a surge of anabolic hormones, primarily insulin which is chronically low on a ketogenic diet. The length of the carb load can vary from 24 to 48 hours and is generally done once a week (usually on the weekend for social reasons). For fat loss, 36 hours is usually ideal since it is very hard to gain much fat during this time period, but 48 hours may be used by those who want to maximize their glycogen stores or are using the diet for muscle gain. It should also be noted that the amount of glycogen in the muscle does not affect how much fat you will lose during the subsequent days as the amount of muscle glycogen only determines how much anaerobic muscle work, such as heavy lifting, can be sustained before amino acids need to be broken down for glucose (recall that the depletion of liver glycogen is what puts you in ketosis irrespective of the size of the muscle glycogen deposits). One subjective way of determining the optimum length of the carb load is to take note of when your body starts to look puffy - that’s when you should revert back to the low-carb phase (something bodybuilders will feel more at home with than, say, powerlifters). Also keep a close eye on your weekly fat loss if you use longer carb loads than 36 hours.
There are two ways of going about the carb-load. The first option is to just plainly eat all carbs that crosses your way while keeping protein and fat reasonable (keep fruit intake minimal though, as fructose does not cause optimal supercompensation due to it being the preferential fuel for refilling liver glycogen). Eat, eat, eat, but when the time period is up, it’s back to the calorie counting. Unscientific as it may seem, this option seems to work well for most people. Not having to count calories and being able to eat whatever (skip the alcohol though) is also a good break that helps give renewed energy for yet another low-carb period. The second option is to optimize the amount eaten by following the following guidelines:
- Carbs: For the first 24 hours, eat 4.5 grams of carbs per pound/10 grams of carbs per kilogram focusing on carbohydrates with a relatively high Glycemic Index (GI). For the second 24 hours, halve the carb intake (i.e. 2.25 grams of carbs per pound/5 grams per kilogram) and focus more on lower GI carbs; if doing a 36 hour carb-load just cut the second 24 hours in half.
- Protein: 1 gram per pound/2.2 grams per kilogram (the end result will be roughly 15% of calories)
- Fat: 15% of calories
For our 209 lbs/95 kg example dieter, a 48 hour carb-load would look like this:
- For the first 24 hours, eat 209 lbs bodyweight * 4.5 grams per pound = 940 grams of carbs (940 grams of carbs * 4 calories per gram of carbs = 3,760 calories), for the second 24 hours eat 940 grams / 2 = 470 grams (470 grams * 4 calories = 1,880 calories).
- Protein is 209 lbs bodyweight * 1 gram per pound = 209 grams (209 grams * 4 calories per gram of protein = 836 calories) for every 24 hours.
- Fat is set at 15% of calories (not grams!). For the first 24 hours: 3,760 calories from carbs + 836 calories from protein = 4,596 calories for the first 24 hours. This is 85% of calories, so 115 percent is 1.15 * 4,596 calories = 5,285 calories out of which fat should comprise 15%, i.e. 0.15 * 5,285 calories = 793 calories, i.e. 793 calories / 9 calories per gram of fat = 88 grams fat. For the second 24 hours: 1,880 calories from carbs + 836 calories from protein = 1.15 * 2,716 calories = 3,123 calories out of which fat should comprise 0.15 * 3,123 calories = 468 calories / 9 calories per gram of fat = 52 grams.
So, the dieter should eat 5,285 calories, 940 grams carbs (71%), 209 grams protein (16%) and 88 grams fat (15%) for the first 24 hours, and 3,123 calories, 470 grams carbs (60%), 209 grams protein (27%) and 52 grams fat (15%) for the second 24 hours. If a 36 hour carb load is desired, the values for the second 24 hours would just be halved and eaten over 12 hours. You may note that the percentages do not add up to precisely 100%; this is not an error in the calculations, but merely the effect of doing away with the decimals by rounding.
Mineral, vitamin and fiber recommendations
It goes without saying that the near lack of vegetables and fruits makes mineral and vitamin (micronutrients) supplementation necessary while on a ketogenic diet. The food choices you make on the ketogenic diet can drastically impact the micronutrient profile of the diet; for example, if plenty of diary products (such as cheese and cream) are eaten calcium will be plentiful, but if they are avoided calcium supplementation would indeed be very necessary. If the carb-load is kept decently healthy some of the micronutrient deficiences of the low-carb days can be made up for, but it would be foolish to count on it. The only way to determine what you need with some precision is to do a mineral and vitamin analysis based on your ketogenic diet food profile, but generally using a generic vitamin and mineral supplement with levels at least at the Reference Daily Intake (RDI) is usually sufficient along with some extra vitamin C (athletes should generally use at least 2,000mg daily) and calcium (600-1,200mg/day) if dairy products are not eaten in large amounts. An extra vitamin B supplement can also be in order, especially if the basic mineral and vitaminsupplement does not contain the whole vitamin B complex. Do make sure that your supplements are sugar free!
A total of 20-30 grams of fiber per day is generally considered optimal. The very low level of fiber present on a ketogenic diet can cause noticable effects in the bathroom, although it is quite common to survive well without any extra fiber once the body gets used to the diet. Nevertheless, some fiber supplementation or ingestion of fiber-rich low-carb vegetables is recommended due to the health benefits of fiber (at least 10 grams/day). The table below, one I made when I first embarked on the ketogenic diet, shows how much of each fiber source must be ingested for 10 grams of fiber. All sources are grouped by the amount of carbs this results in making it easy to rate sources at a glance. All weight measures are in grams. My own personal favorite is a big bowl of cabbage with a greasy garlic dressing on top.
Sources with less than 5 grams of carbs per 10 grams of fiber
| Amount | Carbs | Fat | Protein | Calories | |
| Kale | 232.6 | 4.9 | 2.1 | 4.7 | 58.2 |
| Nettles | 243.9 | 3.2 | 1.7 | 14.4 | 87.8 |
| Mushrooms (canned) | 400.0 | 0.0 | 0.4 | 15.6 | 68.0 |
| Rhubarb | 714.3 | 3.6 | 0.0 | 4.3 | 28.6 |
| Spinach | 769.2 | 3.1 | 3.8 | 14.6 | 107.7 |
5-9 grams of carbs per 10 grams of fiber
| Amount | Carbs | Fat | Protein | Calories | |
| Peas (cooked) | 153.8 | 8.2 | 0.6 | 8.3 | 72.3 |
| Peas (frozen) | 153.8 | 8.2 | 0.6 | 8.8 | 73.8 |
| Hazel nuts | 166.7 | 5.7 | 104.4 | 21.7 | 1058.5 |
| Brussels sprouts | 238.1 | 6.2 | 1.0 | 9.5 | 71.4 |
| Avocado | 368.1 | 6.6 | 81.7 | 15.5 | 831.9 |
| Broccoli | 400.0 | 7.6 | 0.0 | 13.2 | 84.0 |
| Sauerkraut | 454.5 | 8.2 | 1.4 | 6.8 | 72.7 |
| Blanching celery | 555.6 | 7.2 | 0.0 | 0.0 | 50.0 |
| Asparagus (canned) | 666.7 | 8.0 | 1.3 | 15.3 | 106.7 |
| Iceberg lettuce (arctic lettuce) | 833.3 | 6.7 | 1.7 | 8.3 | 75.0 |
| Lettuce (leaves) | 833.3 | 6.7 | 1.7 | 11.7 | 91.7 |
10-15 grams of carbs per 10 grams of fiber
| Amount | Carbs | Fat | Protein | Calories | |
| Peanuts | 123.5 | 10.6 | 60.5 | 30.0 | 715.1 |
| Peas | 181.8 | 10.4 | 0.7 | 10.5 | 90.9 |
| Root celery | 322.6 | 14.8 | 1.6 | 5.5 | 406.5 |
| Aubergine | 400.0 | 12.4 | 0.0 | 2.8 | 60.0 |
| Carrots (boiled) | 400.0 | 13.2 | 0.0 | 2.4 | 64.0 |
| Leek | 476.2 | 11.4 | 1.0 | 13.8 | 109.5 |
| Cauliflower (raw or cooked) | 526.3 | 11.6 | 2.6 | 15.8 | 136.8 |
| Radish | 625.0 | 11.9 | 0.6 | 6.2 | 81.2 |
| Cucumber | 909.1 | 12.7 | 0.9 | 6.4 | 81.8 |
16-20 grams of carbs per 10 grams of fiber
| Amount | Carbs | Fat | Protein | Calories | |
| Lentils (cooked) | 85.5 | 17.2 | 0.3 | 7.7 | 99.8 |
| Green beans | 416.7 | 17.5 | 0.4 | 7.9 | 108.3 |
| Green beans (cooked) | 416.7 | 17.5 | 0.4 | 7.1 | 104.2 |
| Cabbage | 500.0 | 17.0 | 0.5 | 5.5 | 95.0 |
| Red cabbage | 526.3 | 18.4 | 1.1 | 7.4 | 115.8 |
| Chinese cabbage | 833.3 | 18.3 | 1.7 | 10.0 | 113.3 |
21-24 grams of carbs per 10 grams of fiber
| Amount | Carbs | Fat | Protein | Calories | |
| Soy beans (cooked) | 243.9 | 24.1 | 40.5 | 22.0 | 461.0 |
| Red beet (beetroot) | 400.0 | 27.6 | 0.4 | 7.2 | 144.0 |
| Carrots | 416.7 | 22.1 | 0.4 | 3.8 | 108.3 |
| Bell pepper (red) | 526.3 | 23.7 | 2.6 | 6.8 | 147.4 |
| Tomatoes | 714.3 | 24.3 | 1.5 | 6.4 | 135.7 |
Above 25 grams of carbs per 10 grams of fiber
| Amount | Carbs | Fat | Protein | Calories | |
| Onions | 833.3 | 40.0 | 0.0 | 7.5 | 191.7 |
| Kohlrabi | 909.1 | 47.3 | 0.9 | 15.5 | 263.6 |
| Mung beans | 909.1 | 53.6 | 1.8 | 27.3 | 345.5 |
| Zucchini | 928.6 | 40.0 | 1.4 | 11.4 | 185.7 |
Source: Livsmedlens Näringsinnehåll, Finska Folkpensionsanstaltens
publikationer 1989
Training on the Cyclical Ketogenic Diet
Simplistically stated, the goal of a CKD is to deplete muscle glycogen through exercise on the low-carb days (usually 5 days) to a sufficiently low level before refilling glycogen via a 24-48 hour carb-load. It follows that a cyclical ketogenic diet without a sufficient volume of exercise will quickly lead to fat gain as the huge amounts of carbs eaten on the carb-load will quickly cause the glycogen stores to overflow with the excess converted to fat. It is hard to say exactly how much volume is sufficient based on available research on glycogen depletion during weight training, but in his book Lyle McDonald says that a 36 hour carb-load requires about 5 sets of 10-12 reps @ 70% of 1RM (the maximum amount of weight that can be lifted once) per bodypart and a 48 hour carb-load approximately 8 sets per bodypart at the same intensity. Data on other intensity zones are not available, but, say, the standard Westside Barbell powerlifting template ought to be enough. It is also imperative that as large part of all muscle groups in the body is worked since muscle glycogen is local to every muscle. If someone did only bench presses, the legs would hardly be depleted at all. A routine with at least some accessory work to supplement the three powerlifts (or variations of them as in Westside) would seem the best option when done for powerlifting fat loss. As a general rule of thumb, powerlifters should not resort to bodybuilding-style “pumping” when dieting; keep the weights up to retain strength! In sum, lifters following abbreviated routines, such as Heavy Duty, or training infrequently should look at doing a Targeted Ketogenic Diet instead or look into carb-loading less infrequently (such as once every 10-14 days) to accumulate more volume.
Since training speeds up the burning off of liver glycogen, ketosis is established much faster than without exercise. Therefore, a workout is usually schedule at the end of a carb-load (immediately following or the next day). As this is when muscle glycogen levels are at their highest, this should be the most demanding workout of the week and should involve the largest muscle groups of the body. Bodybuilders usually find that the supercompensated glycogen stores with all the associated water will lead to an unbelievable pump for this workout. An hour of low-intensity aerobics (below 65% of maximum heart rate) is even more effective and can cause ketosis to develop in a matter of hours following an overnight fast, but personally I don’t see why a strength athlete should waste the best opportunity for training with aerobics. Each to his or her own I guess. Without exercise, ketosis is usually developed within three days, with moderate volume weight training within about 1-2 days and with an hour of low-intensity aerobics within a few hours.
As the week goes by and the various muscles are stressed directly or indirectly in previous workouts, the more of a performance hit will you experience in later workouts. Since, again, muscle glycogen is only depleted in a particular muscle when that muscle is taxed at sufficient intensity, a powerlifter should find that a decent second max effort day can be done reasonable well as long as the involved muscle groups have not been extensively taxed earlier. However, if that workout takes place late during the low-carb week, performance will definitively suffer. To maximise the time in ketosis, doing the second workout the day following the first workout is ideal if the routine and body can take it.
A second consideration is that muscle glycogen supercompensation is optimal only if the carb-load is begun within two hours after the muscle has been worked. In other words, only the muscle groups heavily taxed in the workout immediately preceeding the carb-load will be optimally supercompensated. Theoretically, this would point to a full-body workout with reps kept at perhaps 10-12 would be the best way to ensure supercompensation of most muscle groups (for powerlifters, this could be an accessory day). It may not be ideal on paper, but in practice many people find that they achieve good results without worrying about the depletion workout being a full-body one. In my opinion, only consider a full-body depletion workout if it doesn’t destroy your lifting routine, or if it turns out that muscles not worked immediately before the carb-load feel sluggish during the week. Another option is to rotate workouts so that different workouts end the carb-load every week. We will go into specifics below, but carbs also need to be ingested before the workout as being out of ketosis following the workout results in better supercompensation.
In sum, here’s how to set-up training around the diet:
- Plan in one workout to end the carb-load: this is done either immediately following the end of the carb load or the next day. Make this the most demanding workout of the week. The large amount of insulin released during the carb-load generally make many people feel lethargic so training during the same day as the carb-load ends is not always the best for good training intensity (as a sidenote, never train DURING a carb-load as this will royally mess up glycogen resynthesis!). Keep in mind that you should avoid carbs both during and after this first workout of the low-carb week; a carb-rich postworkout drink would refill liver glycogen in a snap!
- Plan in one workout to begin the carb-load: this could be a whole body depletion workout or a regular workout. Approximately five hours before this workout ingest about 25-50 grams of carbs (I like candy and a Jolt cola here, but feel free to experiment with slower carbs as well) to begin upregulating liver enzymes. Two hours before the workout a mix of fructose and glucose should be consumed, again 25-50 grams, to refill liver glycogen and exit ketosis. After this workout begin the carb-load immediately, preferably by consuming fast carbs (such as maltodextrin or anything sugarcentric). Keep fat very low for the first hours to kick-start the carb-load.
- Plan in the rest of the workouts: try not to swear too loudly if this breaks your routine…
- Plan in aerobic training if you must: If you feel like you must do aerobics, keep intensity low. Above roughly 65% of the maximum heart rate, the aerobic activity will start to effectively cut into muscle glycogen stores which means that performance in the weight room is hampered. Due to the low-level of anabolic hormones during the low-carb days recovery is slower during the low-carb days, so be careful to allow muscles involved in the aerobic activity to recover before training them with weights. Personally, I would not do any aerobics at all during a cyclical ketogenic diet and save all my energy (and muscle glycogen) for the weights. Obviously, athletes whose sport relies on aerobic fitness should not follow this example.
Measuring progress
Recall that when glucose is stored as glycogen, every gram of glucose binds to 2.7 grams of water. Then consider that a cyclical ketogenic diet depletes glycogen stores severely before a carb-load is done that leads to supercompensated glycogen stores (about 1.5 times the normal amount of glycogen for a 36 hour carb-load). As the glycogen is burned off, the water it binds to is also lost. These changes are large enough to show up on the scale in a big way, leading to typical fluctuations on the order of 5-10 lbs/2.3-4.5 kg a week depending on the amount of muscle mass the lifter carries and how severe a depletion is achieved during the low-carb weeks (some people have reported up to a weekly variance of 15 lbs/6.8kg!). Glycogen supercompensation lasts about three days if no exercise is done; with the training done on a cyclical ketogenic diet, there is usually a large drop in weight around the third low-carb day following the carb-load with a huge weight gain following the carb-load. Again, this is nothing but water weight and has nothing whatsoever to do with true fat loss!
So, how do you find out if you’ve lost any bodyfat in the middle of this weight fluctuation frenzy? Since glycogen depletion will be very similar at the end of every low-carb phase, the best bet is to hop on the scale before breakfast on the day when the carb-load begins (also take possible caliper and girth measurements then). The degree of supercompensation reached after the carb-load can vary some from week to week, especially if not following the scientific model, but it is also a good idea to weigh yourself on the morning following the carb-load. This will give you a reasonable consistent reading of your bodyweight at its lowest and highest. Use the pre-load result as the main indicator of lost fat as that should be more stable than the one after the carb-load. As an example, if the scale shows 217 lbs/98.4 kg one week and 215 lbs/97.5 kg the next the morning when the carb-load begins, you can with reasonable accuracy determine that you’ve lost 2 lbs/0.9 kg of fat. As your fat level drops, the weight following the carb-load should also drop although not necessarily at the same rate as the pre-load measurements. If you keep track on both of these weights (pre-load, post-load) in some kind of chart, you will have a good view of how the diet is working for you.
Putting it all together: a sample cyclical ketogenic diet
Joe is a 200 lbs/91 kg powerlifter who wants to become leaner while keeping as much of his hard-earned lean body mass and strength as possible. He would start the diet at 13 calories per pound (2,600 calories) with carbs kept initially below 30 grams a day (120 calories) or less. Protein intake is 1 gram per pound (200 grams = 800 calories) for the first three weeks, after which it can be dropped down to about 0.8 grams per pound (160 grams). Fat makes up the rest of the calories (1680 calories = 187 grams of fat). Depending on fat loss, calories are adjusted down (or even up if needed) via manipulating the fat intake to keep weight loss at 1-2 pounds/0.5-1kg per week. Calories for the low-carb days of the first week would thus look like this:
2,600 calories
30 grams carbs (4.6% of calories)
200 grams protein (30.8% of calories)
187 grams fat (64.7% of calories)
Joe wants to do a 36 hour carb-load. He has the options of just eating a boatload of carbs during the first 24 hours and a slightly more normal amount for the last 12 hours while keeping fat and protein intake decent all throughout OR following the more scientific model. Using the scientific model, Joe would consume 4.5 grams of carbs per pound of bodyweight (900 grams = 3,600 calories) for the first 24 hours and half of the 2.25 grams of carbs per pound used for the second 24 hours of a 48 hour carb-load (225 grams = 900 calories). Protein is kept at the same 1 gram per pound (200 grams = 800 calories) with fat making up 15% of the calories (again, these values are halved for the last 12 hours). Joe’s carb-load thus looks as follows:
| First 24 hours | Last 12 hours | |
|
5,060 calories 900 grams carbs (71.1%) 200 grams protein (15.8%) 84 grams fat (15%) |
1,495 calories 225 grams carbs (60.2%) 100 grams protein (26.8%) 25 grams fat (15%) |
Joe wants to carb-load on the weekend, and places his last workout at 11am Saturday morning. The workout lasts roughly 1.5 hours after which the carb-load is immediately begun. The first 5,060 calories should roughly be consumed by noon Sunday with the 1,495 calories consumed before midnight Sunday when the carb-load ends. To ensure consistent results, Joe weighs himself Saturday morning on an empty stomach, which is also when possible skinfold and girth measurements should be taken. If results are not satisfactory, Joe should look closely at the his nutrition diary; did he eat too many carbs (possible hidden in something he didn’t think had any carbs) or excessive protein which could have hampered ketosis (cf. ketostix records)? If yes, he should try to create a more favorable ketogenic ratio (without dropping protein too low!) and perhaps also drop calories moderately. If no, he should drop calories further and perhaps also look into cycling them (i.e. eat less one day, and make up for the loss by adding that to the next day). Or did he do too little training causing the carb-load to fail?
To speed up entry into ketosis, Joe schedules his heavy squat day for Monday and his heavy bench day for Tuesday when he is still fresh. The depletion workout consists of accessory work for both the squat and the bench done at submaximal intensity for reps. Optionally, Joe could do squat accessories on Thursday and bench accessories on Friday (or alternate between doing bench and squat accessories on Friday every other week to maximize recovery). The options and diet constraints are many, which gives Joe a slight headache (this is normal).
The final program looks like this:
Monday: low-carb, heavy squat day. Joe also measures his morning weight on an empty stomach to see how much water weight the carb-load put on his body.
Tuesday: low-carb, heavy bench day (use ketostix to start measuring for urinary ketosis)
Wednesday: low-carb, no training (except perhaps very light restorative or technique work)
Thursday: low-carb, no training
Friday: low-carb, no training
Saturday: Joe gets up at 6am to weigh himself and has 25-50 grams of carbs (5 hours before the workout) before going back to bed. At 9am (two hours before the workout), Joe has 25-50 grams of glucose and fructose (a couple of bananas and a Jolt does the trick) together with some protein and fat. The accessory workout is done between 11am and 12.30pm after which the carb-load is immediately begun.
Sunday: Carb-load until midnight (bed time!)
Before embarking on the program, Joe makes sure to have his cholesterol and skinfolds taken. Since he has a digital camera, he also snaps some “before” pictures to compare the final result against. He also weighs himself and gets the mineral and vitamin supplements he needs along with a low-carb cookbook and ketostix. He even remembers to tell his friends in advance of his diet so they know that they should only throw food surprises his way on the weekend when he can eat pretty much anything (unless Joe is too preoccupied with keeping that too scientific all the way…). And not the least, Joe orders The Ketogenic Diet to make sure he thoroughly understands the diet.
Further reading
We conclude this review with a somewhat cursory link section dealing with many aspects of the diet. Weary from writing a long article, this link section is still somewhat under construction. Other link suggestions are warmly welcome.
Ketogenic diets for seizure control in epileptics
- The Atkins diet, which is very similar to the low-carb days described, has been tried with good success as an alternative to the protein and water-restricted ketogenic diet traditionally used in treating epilepsy. See for example,
Eating Your Way to Seizure Control (good intro based on a study from 2003)
A modified Atkins diet is effective for the treatment of intractable pediatric epilepsy, a study from early 2006.
Cyclical ketogenic diet summaries
- Wannabebig articles by Justin Frank: A good multi-part article series dealing with both the science and application of a cyclical ketogenic diet.
Cyclical Ketogenic Diet, The Science
Application of a Cyclical Ketogenic Diet - An extensive summary by Trainerdan on the Active Low-Carber Forums.
- Eat Like a Man: Test driving the Anabolic diet: This two-part series by a much impressed Chris Shugart is somewhat dated, but represents a good read to how the original Anabolic Diet was to be performed and the claims it made in regards to muscle gain. Part I, Part II
Lyle McDonald articles
As a word of warning, Lyle McDonald has been involved with developing the use of cyclical ketogenic diets for athletes for years and has always been most willing to change is mind whenever science or experience proved earlier views flawed. I cannot emphasize enough that you should really get his book.
- Lyle McDonald BodyOpus Pages: This is pretty much where it all began. Essential reading on Lyle’s experiments and thoughts on BodyOpus. Also contains technical papers on and a FAQ, all worth a read, but do keep in mind that he has since revised some of his standpoints.
- Training on the Cyclical Ketogenic Diet: Effects of Cyclical Ketogenic Diets on Exercise Performance (a copy): This Think Muscle article details how exercise impacts fuel utilization and its hormonal response before making specific recommendations on how to set up training around the diet. Accords with his book and is up to date.
- Carbing Up on the Cyclical Ketogenic Diet: Another required read from Think Muscle, this article is a detailed look at the rationale for a carb load and its implementation. The data presented is essentially the same as in his book and is up to date.
Diet variations
- Bodyrecomposition.com is Lyle McDonald’s personal page where he sells books on various diets, mostly ketogenic in nature (note that most, if not all, of his books are also available through Amazon.com).
- Metabolicdiet.com is home to the low-carb variations Mauro DiPasquale developed following the Anabolic Diet. Includes the Radical Diet (a protein sparing modified fast) and the Metabolic Diet.
- Natural Hormonal Enhancement by Rob Faigin is a lifestyle cyclical ketogenic diet.
- The T-Dawg Diet: Version 2.0 by Chris Shugart and TC: A low-carb diet built around the premise of ingesting some extra carbs around workouts for increased anabolism.
Forums
- C-K-D.com - The Cyclical Ketogenic Diet Message Boards
- Active Low-Carber Forums provides support for a wide-range of low-carb diets, including Atkins and CKD variations.
October 30, 2006
CKD diet week 1: Baselines and tentative goals
 Time to get serious. As you all know, I will be lifting in the first ever virtual meet on Feb 9-11th, 2007. My lifts currently suck (pardon me), especially the bench which is just a teensie weensie bit, as in 0.5 kg/1 lbs, above my bodyweight of 104.5 kg/230 lbs. With that meet being scored by relative strength formula, I feel I am giving away too much by having all this extra lard with me on the platform. Some itsy bitsy leverage benefits aside, the spare tires don’t give much of a hand under the bar. Furthermore, I wouldn’t mind being liberated from my gut, however powerliftish it might be. Don’t think I need the fat anymore to look like I lift weights. Case closed, it’s gotta go!
Time to get serious. As you all know, I will be lifting in the first ever virtual meet on Feb 9-11th, 2007. My lifts currently suck (pardon me), especially the bench which is just a teensie weensie bit, as in 0.5 kg/1 lbs, above my bodyweight of 104.5 kg/230 lbs. With that meet being scored by relative strength formula, I feel I am giving away too much by having all this extra lard with me on the platform. Some itsy bitsy leverage benefits aside, the spare tires don’t give much of a hand under the bar. Furthermore, I wouldn’t mind being liberated from my gut, however powerliftish it might be. Don’t think I need the fat anymore to look like I lift weights. Case closed, it’s gotta go!
The plan is as follows. I embarked on a cyclical ketogenic diet (CKD) 20 weeks out from the meet, on 17 September 2006 to be precise. I will be peaking on the same nine-week Extended Russian Routine I used before the one-man meet in August; this leaves me with eleven weeks of dieting at most, probably only ten as I need a week off before the meet. I could also do the first two weeks of the peaking cycle on the diet before switching to regular calories, but I’m not counting on that just yet. In practice, this means dieting up until the first week of December, then peaking until the first weekend of February and a week off before the meet.
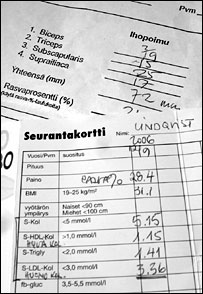
To establish a baseline, I had my cholesterol checked at a local branch of the Finnish Heart Association before starting the diet. I was told I was a rare sight compared to the typical elderly patient with heart disease, but it was cheap and is the only place I know of which doesn’t require seeing a doctor first. After waiting half an hour with Rufus, the results came out as a total fasting cholesterol of 5.15 mmol/l broken up into 3.36 mmol/l of LDL (”bad”) cholesterol, 1.15 mmol/l of HDL (”good”) cholesterol and 1.41 mmol/l of Triglycerides. If we put Anthony Colpo aside for a second in order to blindly stare at the Finnish recommendations, we can see that my total cholesterol (< 5 mmol/l recommended) and LDL (< 3 mmol/l) are slightly elevated while Triglycerides (< 2mmol/l) and HDL (> 1 mmol/l) are where they should be. “Getting rid of a few kilos should solve that easily”, the nurse said. Last time I was on this diet, my total cholesterol increased, but the ratio of HDL to LDL improved markedly which is a good thing; going to be interesting to see how it goes this time around.
Finding someone proficient in wielding calipers to measure bodyfat was much harder. Finally, the front desk at Töölö Gym referred me to Kirsi Halme, a certified personal trainer from the Fitness Academy of Finland. I had to wait for a week due to her being on sick leave, but it was worth it. She promptly received me at 9am in a small room at the gym and with sure hands measured my biceps (19mm), triceps (15mm), subscapularis (25mm) and suprailiac (17mm) for a total of 72mm or 24.4% bodyfat (for fun, she also checked it electronically resulting in 23.5%). It took less than ten minutes and only put me back 7 euros. Seems like I am not only packing it in the form of spare tires, I also have quite a formidable coating on my back as evidenced by the subscapularis spot. And no, I didn’t have Rufus’s bodyfat checked.
Time for some math. 24.4% bodyfat at 104.5 kg/230 lbs means I carry 79 kg/174 lbs lean body mass (LBM) and 25.5 kg/56 lbs fat. The Body Mass Index (BMI) puts me at 31.2 and smacks an obesity stamp across my forehead. The absurdity of applying the BMI on weight trained individuals with their above average muscularity becomes obvious when we consider that in order to reach a “normal weight” of 20-25 BMI, I should weigh 67-84 kg/148-185 lbs at my height of 183 cm/6 feet. The lower end is 12 kg/26 lbs BELOW my lean body mass (-17% bodyfat?!) and the upper end would put me at 5.9% bodyfat, well below the recommended healthy range of 8-19%. If we consider 15-18% bodyfat to be normal, someone falling into this BMI bracket would be carrying 57-69 kg/126 lbs-152 lbs LBM. Given the average of 63 kg/139 lbs LBM, I would be carrying roughly 16 kg/35 lbs more muscle than the average normal weight man my height. Granted, this is a very sketchy picture at best, but it does give some indication of where I stand in the grand scheme of humanity.
If we presume eleven weeks of dieting and an average weekly fat loss of 0.7 kg/1.5 lbs per week, I would drop around 8 kg/17 lbs, i.e. down to 96.5 kg/213 lbs at 18% bodyfat assuming zero muscle mass loss (reality will bite). I could then easily shed about 2.5 kg/5.5 lbs more for the meet weigh-in by normal water weight manipulation, putting me at 95 kg/213 lbs for the meet when allowing for a realistic 1 kg/5 lbs weight gain during the peaking cycle. With a Wilks score of 236.4319 for my current PR total of 395 kg/869 lbs at 104.5 kg/230 lbs, I would need to get a total of about 347.5 kg/766 lbs for the same score at 95 kg/213 lbs. I have a hard time seeing my total plunge 47.5 kg/105 lbs, so, increasing relative strength would appear to be a given even when allowing for decreased weight on the bar. Furthermore, the peaking cycle is likely to restore at least some of my strength. As a point of reference, replicating my current total at 95 kg/230 lbs would amount to a Wilks score of 245.7011, a 9.2692 point gain. If I were to take the other route of adding strength instead of dropping weight, it would take a total of about 410 kg/904 lbs total at 104.5 kg/230 lbs to equal that, i.e. a 15 kg/33 lbs gain (say, an 145 kg/320 lbs squat, 110 kg/243 lbs bench and 155 kg/342 lbs deadlift). When push comes to shove, I would be happy with weighing in at no more than 96 kg/212 lbs and posting a Wilks score of at least 240, but the truth be told, in my dreams I am breaking the 400 kg/882 lbs RAW barrier. Long term, I want to start keeping my bodyfat between 15 and 18% so that I could easily be reasonable competitive at a meet, real or virtual, without having to diet extensively. Given my current LBM, this would mean a training weight of roughly 90-93 kg/198-205 lbs and competing at the upper end of the 90 kg/198 lbs weight class. Draconian as it may be, another diet is needed after the meet to put me down at 15% bodyfat. That’s long-term planning for you.
More detail on how I am setting up my dieting training program, a modified version of the Pure Power Mag 16-week Squat Routine, will appear shortly in the luminous guise of the first weekly summary in a looong while. Hold on to your hats if you have ‘em, a backblogging storm is brewing. If it wasn’t obvious, this entry should have appeared in September, at the time of press I am already at week 7 of dieting. Sheesh.